Technology
Development of DRhQ
A novel, differentiated dual-mechanism biologic targeting the MIF/CD74 pathway to block neuroinflammation and promote neuroprotection.
RTL-labeled monocyte · fluorescence microscopy
A novel, differentiated dual-mechanism biologic targeting the MIF/CD74 pathway to block neuroinflammation and promote neuroprotection.
RTL-labeled monocyte · fluorescence microscopy
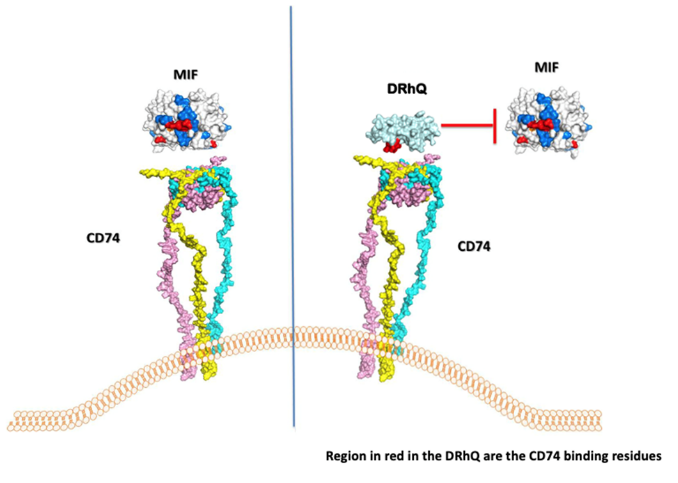
Artielle's novel, differentiated dual mechanisms (1) competitively inhibit binding and downstream signaling of macrophage migration inhibitory factor (MIF) through its major CD74 receptor on monocytes, and (2) CD-74+ pathogenic, effector memory CD4+ and CD8+ T cell activation leading to reduced inflammation.
DRhQ competitively inhibits binding and downstream signaling of macrophage migration inhibitory factor (MIF) through its major CD74 receptor on monocytes and CD4+ and CD8+ effector memory T cells. MIF is a key inflammatory cytokine elevated in MS and following methamphetamine use.
These actions reverse the chemotactic gradient attracting peripheral inflammatory cells to the site of CNS injury and, further, promote apoptosis of these destructive infiltrating cells.
In neurodegenerative animal models, this results in local reprogramming of microglial cells and astrocytes to produce a neuroprotective effect. In cancer models, DRhQ can potentially reduce tumor cell viability and promote tumor immunity.
The platform is based on molecules derived from a portion of the MHC II molecule — specifically the DRα1(L50Q) portion — tethered to a peptide (Myelin Oligodendrocyte Glycoprotein, MOG) that conveys both disease specificity and conformational stability to the molecules. The fact that both the components in DRhQ are conserved in humans as "self" reduces the likelihood of inflammatory neutralizing immune responses after treatment.
DRhQ shows efficacy in animal and cell-based models for multiple sclerosis, methamphetamine use disorder, stroke, melanoma, and triple negative breast cancer. The inhibition of the downstream signaling through the CD74 receptor provides measurable biomarkers that can be used for clinical development.
Artielle has completed a double-blind, placebo-controlled, Phase I dose escalation study of the safety of a single intravenous (IV) dose of RTL1000 — the first-generation biologic — in MS patients. The drug was administered to six cohorts (escalating doses ranging from 2mg to 200mg) and all subjects were followed over 28 days. The primary endpoint was met and a maximum tolerated dose was established, paving the way for the next-generation molecule DRhQ. The DRhQ molecule is able to treat a larger patient population because it lacks the DR2β1 domain present in RTL1000 – making it a superior biologic to the first-generation molecule.